Tackling Complex Conditions with Precision and Insight
For Accountable Care Organizations (ACOs), chronic care management isn’t optional; it’s essential. With rising costs, aging populations, and value-based contracts that reward outcomes over volume, ACOs are under more pressure than ever to deliver better care for patients with complex needs.
But here’s the catch: chronic disease doesn’t follow a playbook. It’s messy, unpredictable, and deeply personal. So how do ACOs scale care that feels customized, proactive, and efficient—all at once? That’s the real puzzle. In this post, we’ll dig into the proven strategies and digital innovations that are finally moving the needle on ACO chronic care management.
Whether you’re leading an ACO, part of a care team, or simply passionate about transforming healthcare, this is where scalable chronic care starts to make sense. Let’s get into what’s working—and what’s next.
The 7 Most Common Challenges in ACO Chronic Care Management
Managing chronic disease isn’t just about getting someone to take their meds. It’s about building a health system that supports people every day, not just when they show up at the doctor’s office. For Accountable Care Organizations (ACOs), that’s a big lift—and it comes with serious hurdles.
Here are the seven most common problems ACOs run into when trying to manage chronic illness at scale:
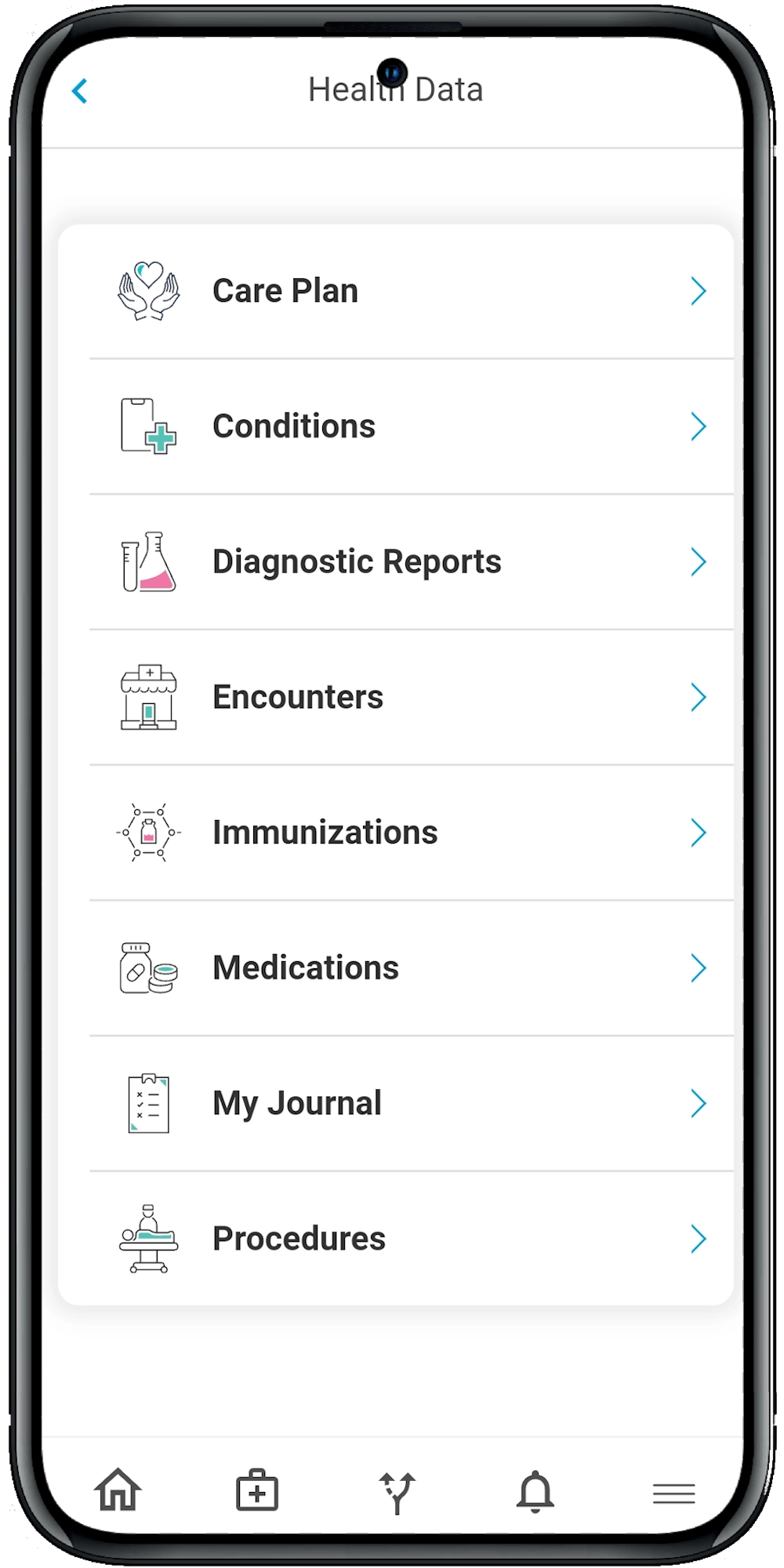
- Scattered patient data. Health records spread across different EHRs make it hard to get a full view of the patient.
- Low patient engagement. Many patients don’t understand their conditions, forget instructions, or struggle to follow care plans.
- Clunky care coordination. Disconnected workflows between providers, case managers, and specialists create confusion and inefficiency.
- Lack of real-time feedback. Without timely data, providers often miss red flags until it’s too late.
- Administrative overload. Managing documentation, compliance, and reporting drains time and energy from direct patient care.
- Inconsistent execution of care plans. Protocols aren’t always followed the same way across teams, leading to gaps in care.
- Post-discharge care gaps. Delayed or missed follow-up after hospital stays contributes to avoidable readmissions (Hewner et al., 2016).
So What Actually Works? Proven Approaches from Successful ACOs
The good news? We’re not guessing anymore. Decades of data, including recent studies and real-world implementations, have shown what does work when it comes to ACO chronic care management.
Let’s walk through a few evidence-backed strategies.
1. Digital Home Visits and Remote Monitoring
The old-fashioned house call is back—only now, it’s digital. ACOs that conducted home visits within 72 hours of discharge were more likely to reduce readmissions and uncover risks early, like fall hazards or medication errors (Fraze et al., 2019).
Even better? With today’s technology, these check-ins can happen remotely.
Digital home visit features that make a difference:
- Medication reconciliation via video or app
- Remote monitoring of vitals like blood pressure or glucose
- Environmental assessments through virtual walkthroughs
- Caregiver engagement and coaching
The takeaway? You don’t need a van and a clipboard. You need a platform that puts “eyes in the home” virtually—and reliably.
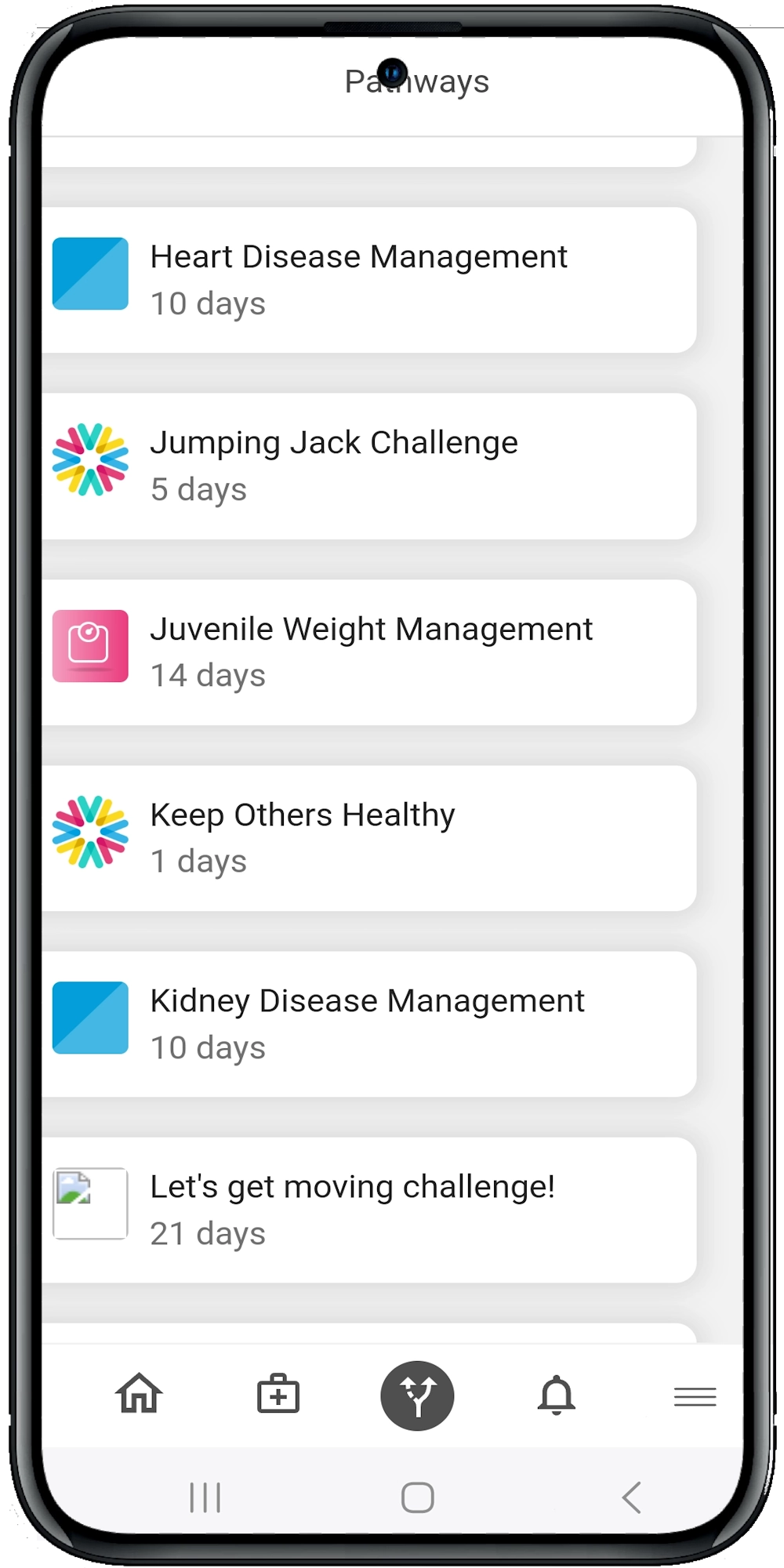
2. Standardized Care Pathways—Delivered Digitally
A major challenge in ACO chronic care management is making sure everyone is on the same page. That’s why digital care pathways are gaining momentum. These are structured, interactive programs that walk patients through what to do each day, week, or month.
Platforms like Calcium offer hundreds of condition-specific digital pathways—everything from diabetes and hypertension to asthma and post-op recovery.
Here’s what digital pathways typically include:
- Daily reminders for meds, exercise, and check-ins
- Step-by-step guidance based on diagnosis
- Auto-adjusting content based on patient feedback or health data
- Alerts to care teams if a patient falls off track
It’s like giving every patient a personal health GPS—and every provider a dashboard to track their route.
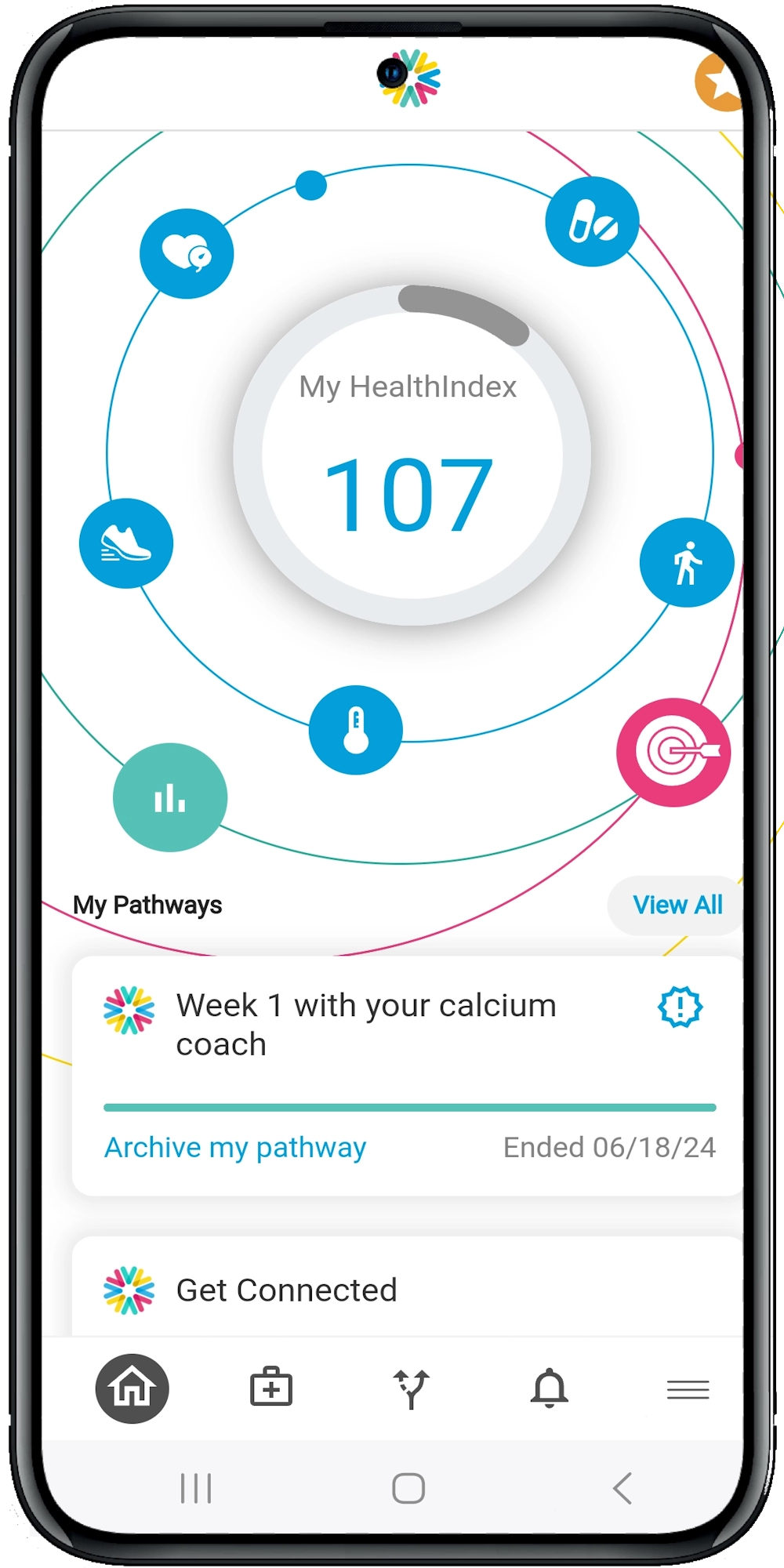
3. Real-Time Health Data and Proactive Alerts
Catching health issues early is what keeps people out of the ER. But you can’t do that if you’re flying blind.
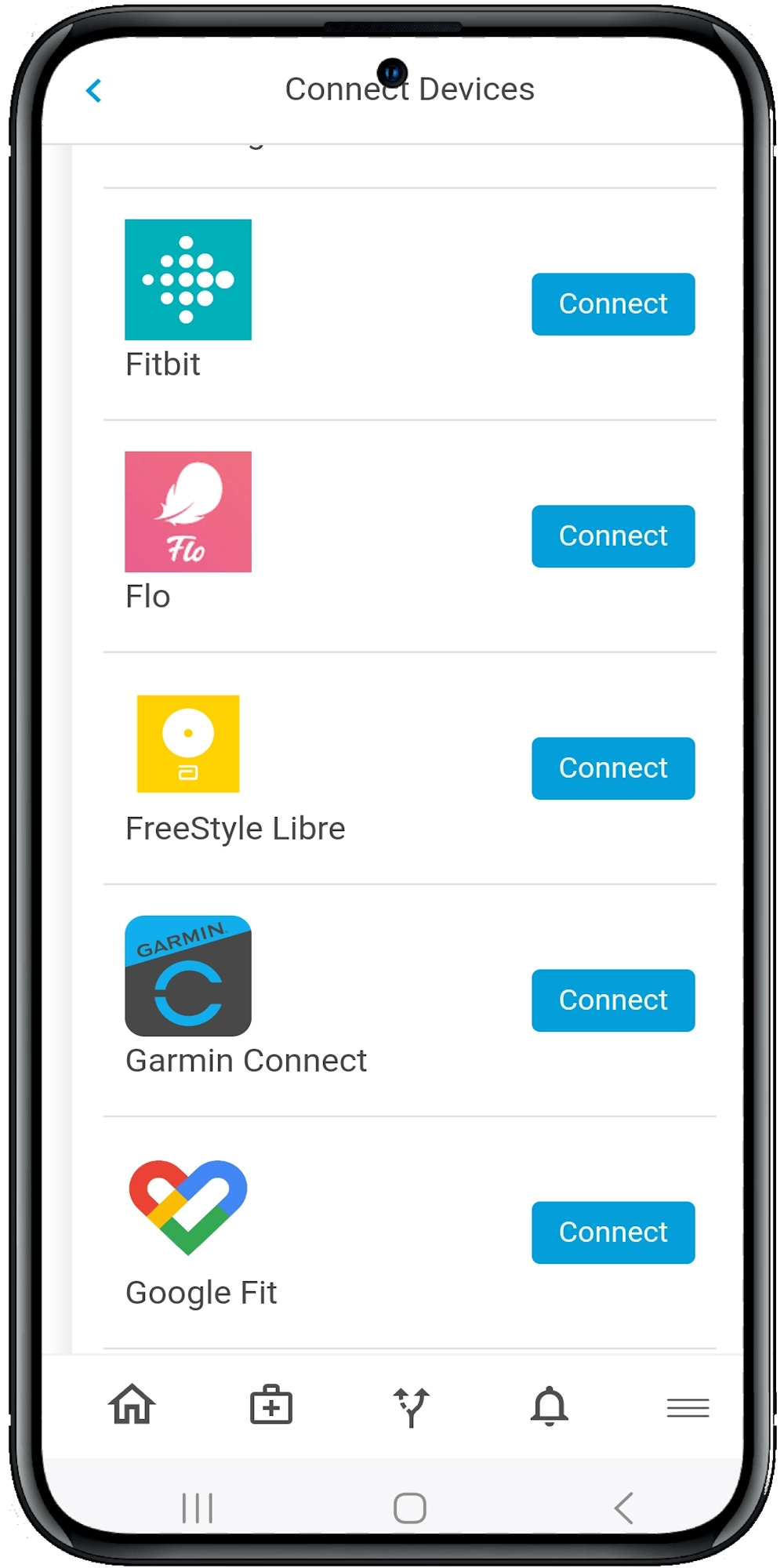
Wearables, at-home devices, and mobile apps now let patients feed in data 24/7. With the right tools, ACOs can monitor trends, detect red flags, and reach out before a situation turns critical.
Real-time data can include:
- Heart rate variability
- Blood glucose levels
- Weight fluctuations
- Mood and mental health self-reports
- Symptom journaling (like shortness of breath or fatigue)
Calcium’s Super App integrates this kind of data automatically—and triggers alerts to care managers when something’s off.
It’s not just reactive care. It’s predictive care.
4. Intelligent Risk Stratification and Population Segmentation
You can’t treat every patient the same way. That’s why smart ACOs use data analytics to segment their populations and prioritize high-risk individuals.
A 2020 study on ACO-affiliated hospitals found that those using multiple payment models, including shared savings and capitation, implemented care coordination strategies more widely—especially around high-risk patient identification (Anderson & Chen, 2019).
With AI-driven tools, ACOs can:
- Identify “rising risk” patients before they hit crisis mode
- Match patients to the right care team members
- Adjust care plans dynamically as needs evolve
This kind of precision isn’t just nice to have. It’s how you scale chronic care without losing sight of the individual.
5. Embedding Behavioral Health into Primary Care
You can’t separate the mind from the body. Behavioral health plays a huge role in chronic disease management. Depression, anxiety, and substance use can all interfere with treatment adherence and lifestyle changes.
The problem? Behavioral health is often siloed.
Platforms like Calcium bridge that gap by embedding behavioral health assessments and pathways directly into the primary care experience. That means:
- Regular screening for depression or anxiety
- Integrated care plans that include mental health goals
- Access to digital CBT tools, mindfulness prompts, or coaching
- Alerts when behavioral risk factors rise
Addressing mental health isn’t optional. It’s foundational to any successful ACO chronic care management strategy.
6. Automating the Back-End: Documentation, Reporting & Compliance
Care teams shouldn’t have to choose between seeing more patients and meeting quality metrics. Automating administrative tasks frees up time and reduces burnout.
Here’s what automation looks like in practice:
- Auto-documenting patient actions in care pathways
- Generating real-time reports for MIPS or HEDIS measures
- Tracking compliance with treatment plans
- Simplifying data exports for ACO dashboards
Calcium’s backend tools do all of this in the background—so providers can focus on people, not paperwork.
The Wrap
Scaling chronic care management isn’t just a lofty goal—it’s an urgent necessity for ACOs striving to improve outcomes, reduce costs, and truly support patients living with chronic conditions.
All the research, studies, and pilots agree: ACO chronic care management can work at scale—but only when supported by the right digital foundation (Kaufman et al., 2019). From real-time monitoring to automated care plans, the playbook is ready. It’s now about execution.
The right digital tools can turn those challenges into opportunities for smarter, more connected care. It’s no longer enough to react to illness; success in value-based care depends on being proactive, personalized, and data-driven at every step.
That’s where the Calcium digital health platform comes in. From real-time patient engagement to automated care pathways and seamless coordination, Calcium is built to help ACOs manage chronic disease at scale—without compromising the human touch.
Reference
- Ouayogodé, M. H., Mainor, A. J., Meara, E., Bynum, J. P. W., & Colla, C. H. (2019). Association Between Care Management and Outcomes Among Patients With Complex Needs in Medicare Accountable Care Organizations. JAMA Network Open, 2(7), e196939. https://doi.org/10.1001/jamanetworkopen.2019.6939
- Fraze, T. K., Beidler, L. B., Briggs, A. D. M., & Colla, C. H. (2019). “Eyes In The Home”: ACOs Use Home Visits To Improve Care Management, Identify Needs, And Reduce Hospital Use. Health Affairs, 38(6), 1021–1027. https://doi.org/10.1377/hlthaff.2019.00003
- Anderson, A. C., & Chen, J. (2019). ACO Affiliated Hospitals Increase Implementation of Care Coordination Strategies. Medical Care, 57(4), 300–304. https://doi.org/10.1097/mlr.0000000000001080
- Kaufman, B. G., Spivack, B. S., Stearns, S. C., Song, P. H., & O’Brien, E. C. (2019). Impact of Accountable Care Organizations on Utilization, Care, and Outcomes: A Systematic Review. Medical Care Research and Review, 76(3), 255–290. https://doi.org/10.1177/1077558717745916
- Hewner, S., Casucci, S., & Castner, J. (2016). The Roles of Chronic Disease Complexity, Health System Integration, and Care Management in Post-Discharge Healthcare Utilization in a Low-Income Population. Research in Nursing & Health, 39(4), 215–228. https://doi.org/10.1002/nur.21731