Making Healthcare Work Smarter for Patients and Providers
Imagine walking into a doctor’s office where your entire care team already knows your health history, current medications, and even how well you’ve been sleeping—all without you saying a word. That’s not science fiction—it’s the promise of value-based care, and Accountable Care Organizations (ACOs) are leading the charge.
In a system that’s long rewarded quantity over quality, ACOs are flipping the model to focus on outcomes, prevention, and smarter collaboration. But as healthcare costs rise and disparities deepen, the pressure is on: ACOs must deliver more than good intentions. They need to prove they can improve health while reducing costs—and do it at scale.
So, what’s helping the most effective ACOs succeed where others stall? And how can digital tools give them the edge they need? Let’s take a closer look at why ACO value-based care is more than a trend—it’s a necessary evolution, and the right technology may be its best ally.
What Makes ACOs Tick in a Value-Based World?
Success in ACO value-based care isn’t about just switching payment models. It’s about rethinking how care is delivered, how patients are supported, and how outcomes are achieved—together.
ACOs are designed to meet these demands head-on. But they’re not immune to real-world challenges. Let’s break down what makes ACOs work and how they overcome the very hurdles that hold many healthcare organizations back.
1. Strong Primary Care is the Command Center
One of the biggest barriers in U.S. healthcare today is fragmented, reactive care. Patients often bounce between providers without clear handoffs or a quarterback to lead the charge. That’s where ACOs shine.
At the heart of every successful ACO is a strong primary care network. These providers are the frontlines—monitoring patients regularly, managing chronic diseases, and catching problems before they escalate. Primary care in an ACO isn’t just routine—it’s strategic. According to a JAMA study, ACOs anchored by robust primary care are more likely to lower costs and meet quality targets (Heiser et al., 2019).
But here’s the challenge: primary care is often underfunded and overstretched. ACOs flip the script by shifting financial incentives away from volume and toward outcomes. This model allows primary care teams to invest in care coordinators, health coaches, and remote monitoring—things they couldn’t justify under fee-for-service.
2. Coordinated Care Reduces Chaos
Another major issue? Disconnected care. Without shared systems, patients see multiple providers who don’t talk to each other. It’s like being passed from one department to another with no map. This leads to duplicated tests, conflicting medications, and unnecessary ER visits.
ACOs are built to solve that. By design, they bring together providers across specialties, hospitals, and care settings under one umbrella. Everyone’s incentivized to collaborate because their performance is judged collectively. When done right, care becomes continuous and connected—exactly what value-based care needs.
Still, care coordination is no walk in the park. Many ACOs struggle with real-time communication tools and data access. But the best ones build out infrastructure—shared records, regular care team huddles, and integrated discharge planning—to fill these gaps. It’s not just about reducing waste; it’s about improving experience for both patients and providers.
3. Data Isn’t Optional—It’s the Backbone
Ever try to steer a ship with no radar? That’s what managing a population without data feels like. One of the key reasons traditional systems fail in value-based models is the lack of timely, actionable information.
ACOs approach data differently. They need to know who’s at risk, who’s slipping through the cracks, and who needs immediate attention. The most successful ACOs use analytics to:
- Stratify patients by risk
- Monitor hospitalization patterns
- Identify gaps in care
- Track outcomes by race, income, or zip code
But here’s the rub: many ACOs are still wrangling data from disconnected EHRs, payer feeds, and health IT systems that don’t talk to each other. Even with those hurdles, ACOs are better positioned to centralize and act on this data because their payment model rewards insight. They’re not just collecting data—they’re using it to make real-time decisions that improve outcomes (Foster et al., 2024).
And with CMS pushing programs like ACO REACH, which requires tracking and addressing health disparities, that data becomes even more mission-critical for ACO value-based care strategies.
4. Patient Engagement is the Hidden Engine
Most people assume improving health is all about what happens in clinics or hospitals. But the truth? Up to 80% of outcomes are driven by what patients do (or don’t do) outside the office—what they eat, whether they move, if they take their meds, and how they manage stress.
That’s where the traditional system breaks down. Once the visit is over, the follow-through is often left to chance. ACOs know this, and they work to fill that void with high-touch, high-tech strategies.
But let’s be real: keeping patients engaged isn’t easy. Many face barriers like low health literacy, limited internet access, or competing life priorities. ACOs overcome these by:
- Assigning care navigators or health coaches
- Creating culturally relevant education materials
- Using telehealth and mobile tools to stay connected
- Offering behavioral health and social services under one roof
When ACOs treat patients as partners—not just recipients of care—they unlock better adherence, better outcomes, and lower total costs. That’s ACO value-based care in action.
5. Aligned Incentives Make the System Work for Everyone
Let’s not forget one of the most basic flaws of fee-for-service: it rewards doing more, not doing better. In that model, a provider gets paid for every test, visit, and procedure—regardless of whether it helps the patient.
ACO value-based care flips that logic. Instead of getting paid more when a patient returns to the ER, providers get rewarded when that ER visit is prevented in the first place. That changes everything.
Now, this doesn’t come without tension. Many ACOs still operate in hybrid models, juggling fee-for-service revenue with value-based contracts. And downside risk—where ACOs can lose money for poor performance—can make some providers hesitant.
But here’s what we’ve learned from research like the NEJM’s MSSP study: ACOs that embrace shared savings, especially independent primary care groups, tend to see the most success. They reduce unnecessary inpatient and post-acute care and reallocate resources toward prevention and community-based care (McWilliams et al., 2016).
Moreover, the growth of ACOs has been significant. By the first quarter of 2018, there were 1,011 ACOs covering approximately 32.7 million patients across the U.S., indicating a substantial shift towards value-based care models (Muhlestein et al., 2018).
When incentives align with patient outcomes, everyone wins.
How Calcium Supercharges ACO Performance
So how do ACOs go from good to great? The answer lies in digital transformation. And Calcium’s digital health platform is built specifically to support ACOs’ value-based care.
Here’s how:
Centralized Health Data = Complete Visibility
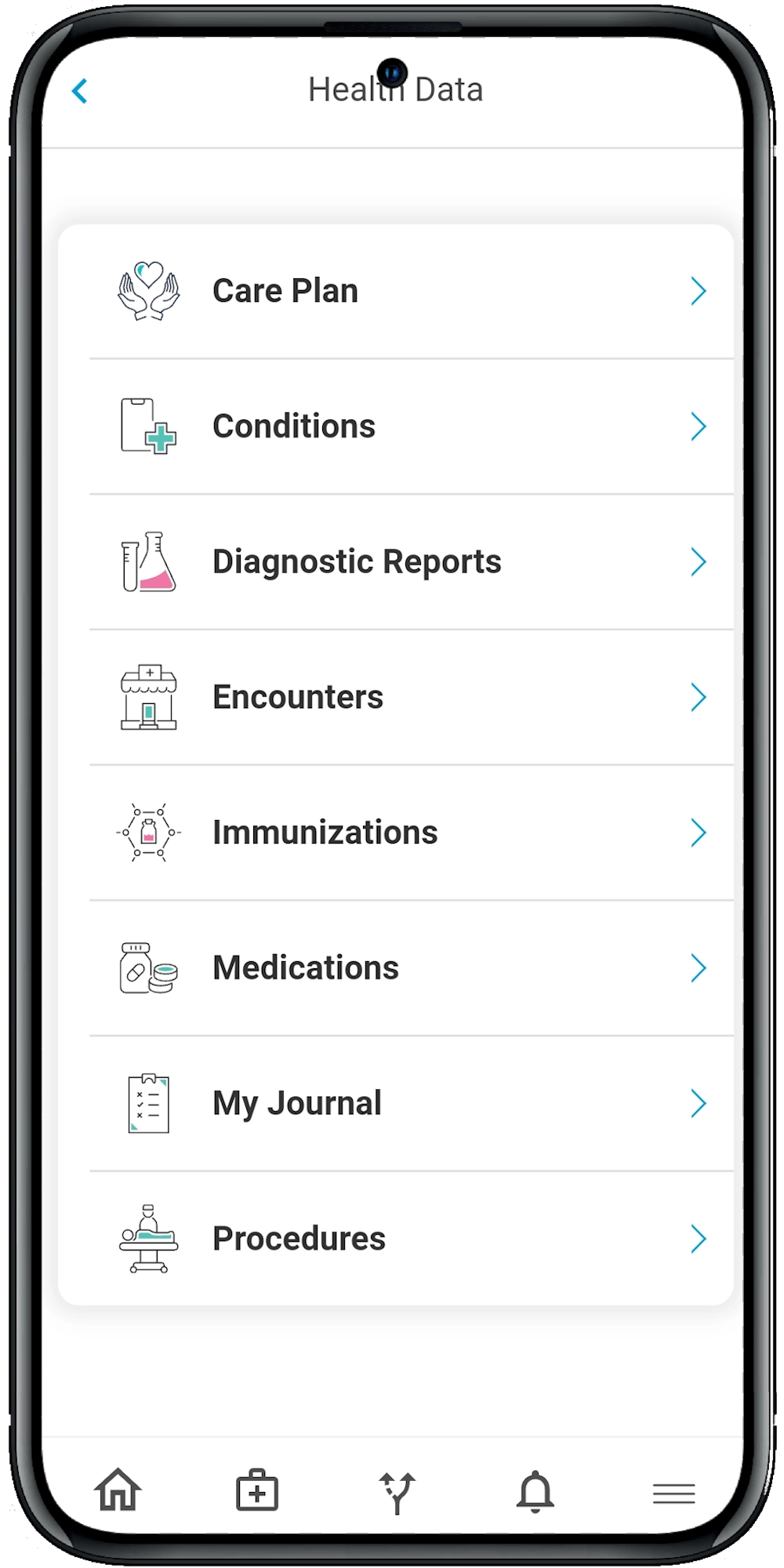
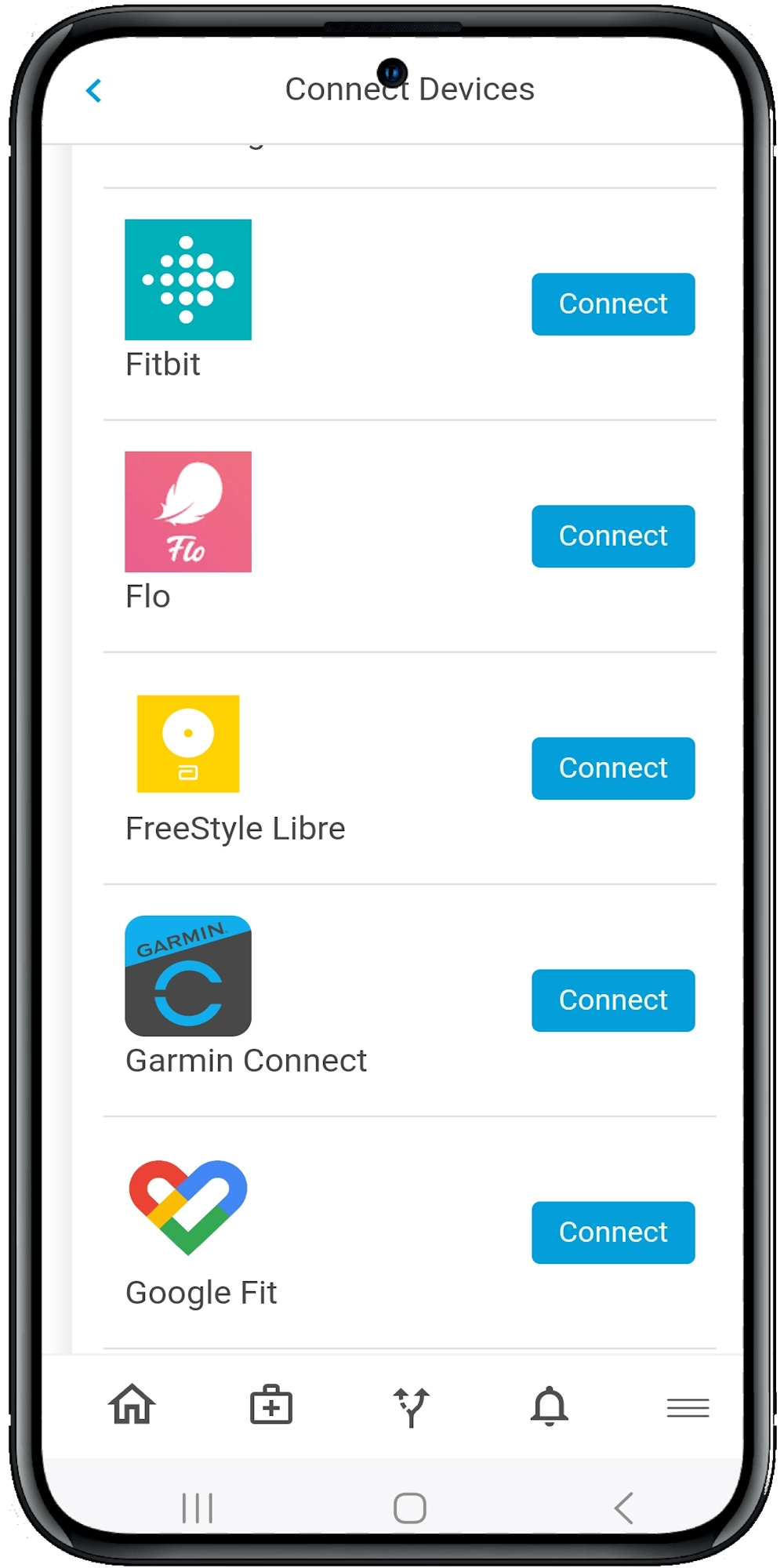
Calcium pulls in data from electronic health records, wearables, fitness apps, lab results, and more—creating a unified health profile for each patient. This is especially useful for ACOs dealing with fragmented systems and inconsistent data feeds. With Calcium Core, care teams can finally get the full picture in one place.
AI-Powered Digital Pathways Keep Patients on Track
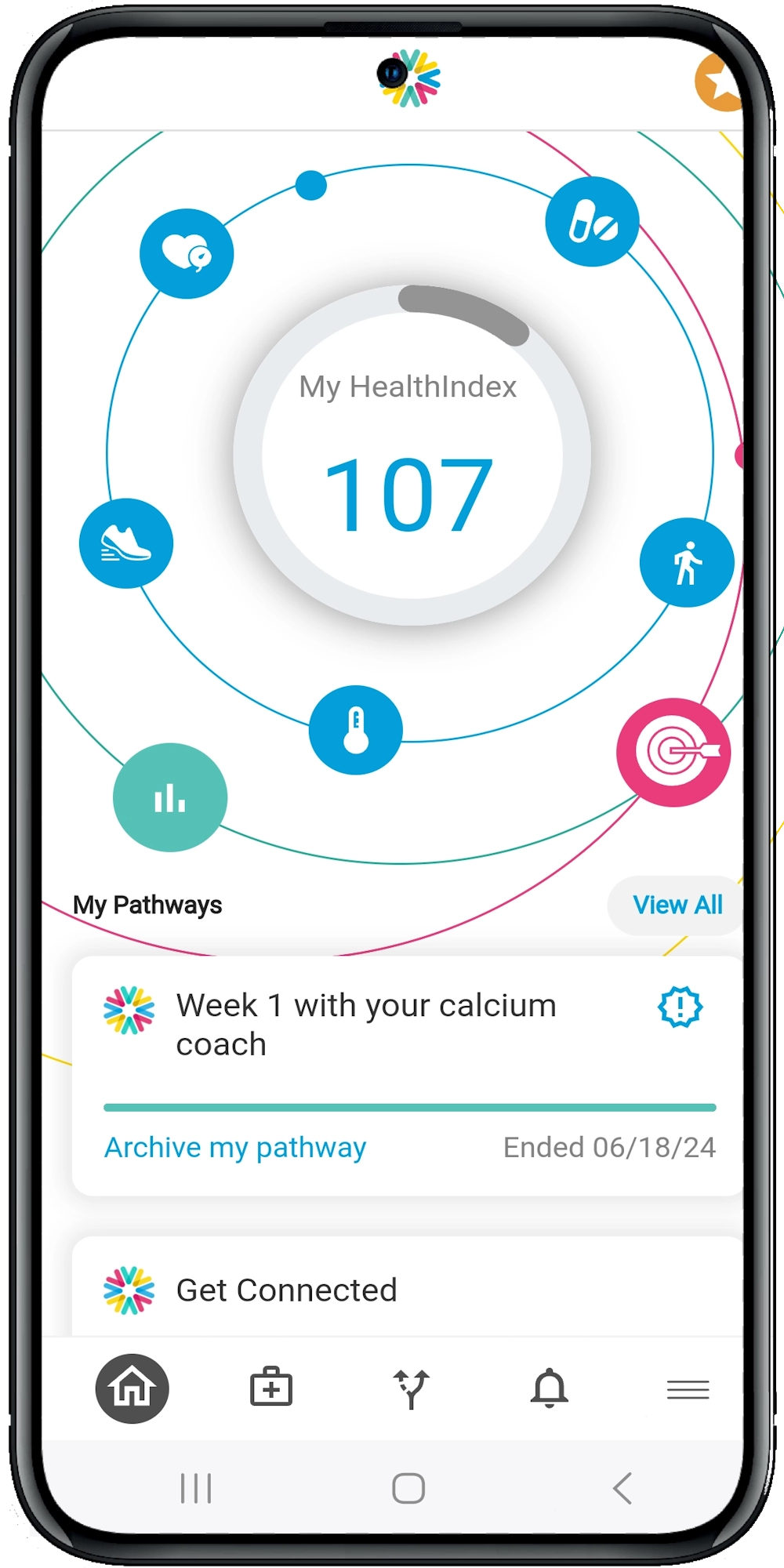
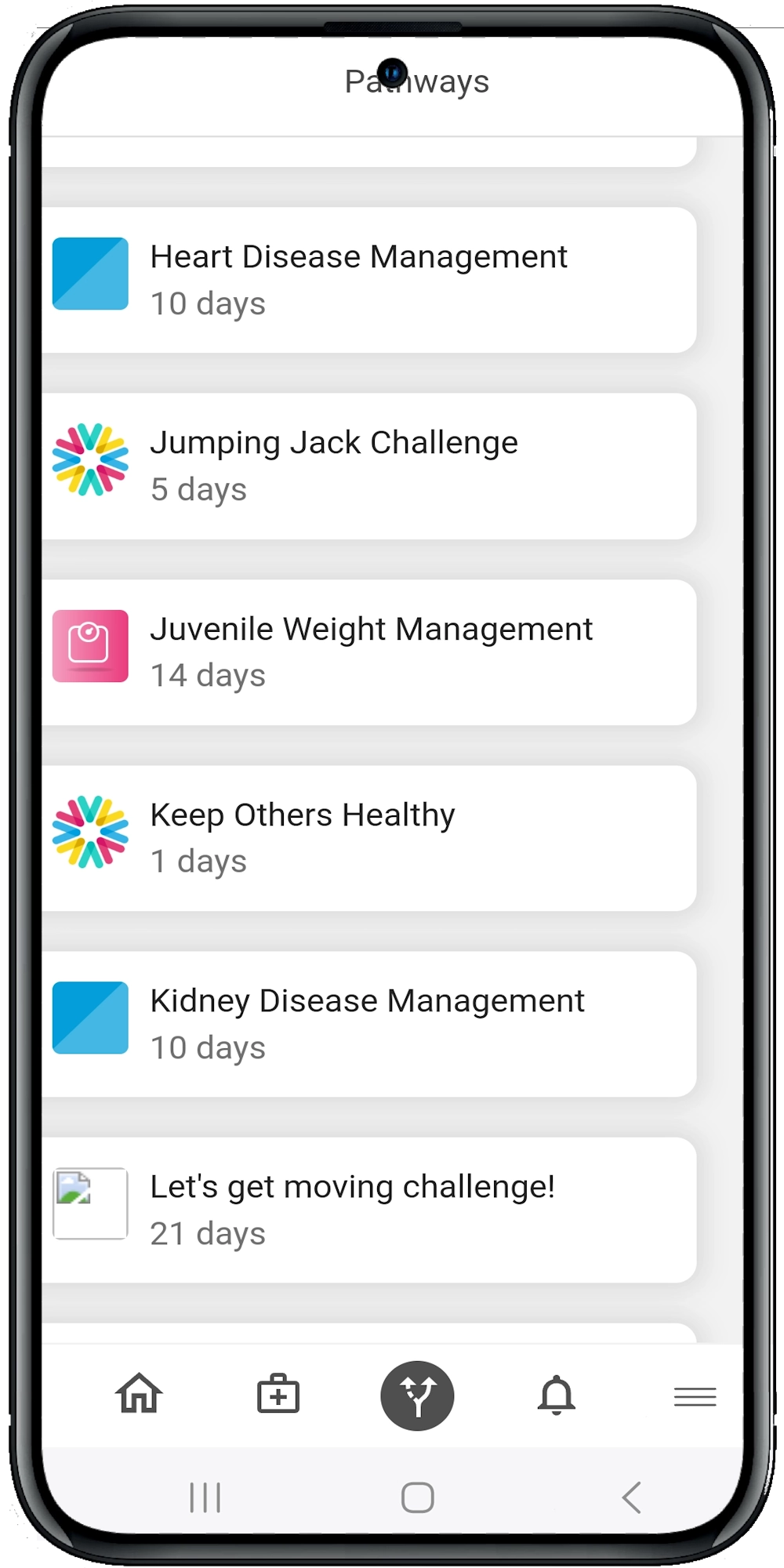
Through the Calcium Super App, ACOs can assign tailored digital care plans—known as pathways—that help patients manage chronic conditions, prep for surgery, or stick to wellness goals. These plans send daily reminders, collect symptom data, track vitals, and offer real-time feedback. Patients stay engaged. Providers stay informed.
Health Equity at the Forefront
With CMS requiring health equity plans in models like ACO REACH, Calcium helps ACOs stratify data by SDOH factors—race, income, geography—and flag disparities. This makes it easier to tailor interventions, allocate resources, and prove compliance with federal equity goals.
Real-Time Alerts Prevent High-Cost Episodes
Whether it’s a spike in blood pressure or a skipped appointment, Calcium’s analytics engine flags problems early—so care teams can intervene before things escalate. This means fewer ER visits, lower readmission rates, and better population health.
Seamless Collaboration Across Care Teams
Providers, care coordinators, behavioral health specialists, and even family members can communicate through secure, in-app messaging. Everyone stays in sync, and patients feel fully supported.
The Wrap
The future of healthcare hinges on our ability to deliver better outcomes without breaking the bank—and ACO value-based care is paving that path. But to truly succeed, ACOs need more than good policies and clinical expertise—they need digital tools that make proactive, patient-centered care possible.
From streamlining care coordination to empowering patients in their daily health decisions, platforms like Calcium are turning those goals into measurable results. Whether you’re managing chronic disease populations, trying to reduce readmissions, or working to close care gaps across diverse communities, the right technology can make all the difference.
Reference
- Muhlestein, D., Saunders, R. S., de Lisle, K., Bleser, W. K., & McClellan, M. B. (2022, December 2). Growth of value-based care and accountable care organizations in 2022. Health Affairs Forefront. https://doi.org/10.1377/forefront.20221130.22253
- Muhlestein, D., Saunders, R. S., Richards, R., & McClellan, M. B. (2018, August 14). Recent progress in the value journey: Growth of ACOs and value-based payment models in 2018. Health Affairs Forefront. https://doi.org/10.1377/forefront.20180810.481968
- McWilliams, J. M., Hatfield, L. A., Chernew, M. E., Landon, B. E., & Schwartz, A. L. (2016). Early Performance of Accountable Care Organizations in Medicare. New England Journal of Medicine, 374(24), 2357–2366. https://doi.org/10.1056/nejmsa1600142
- Foster, N., Durand, D. J., Johnson, P. T., Glover, M., & Narayan, A. K. (2024). Emerging Value-Based Care Payment Mechanisms to Reduce Health Inequities: The ACO REACH Model. Journal of the American College of Radiology. https://doi.org/10.1016/j.jacr.2024.05.007
- Heiser, S., Conway, P. H., & Rajkumar, R. (2019). Primary Care Selection. JAMA, 322(16), 1551. https://doi.org/10.1001/jama.2019.14190